Tardive dyskinesia (TD) and drug-induced parkinsonism (DIP) are common movement disorders experienced by patients taking dopamine receptor blocking agents, the active agent in many antipsychotic drugs.1-3 While the symptoms of TD and DIP may have some similarities, these disorders are caused by opposing mechanisms, and treatment for one can exacerbate the symptoms of the other.1,2 It is, therefore, imperative to be able to effectively distinguish between the two. Understanding the causes of TD and DIP can help contextualize their treatment.1,4
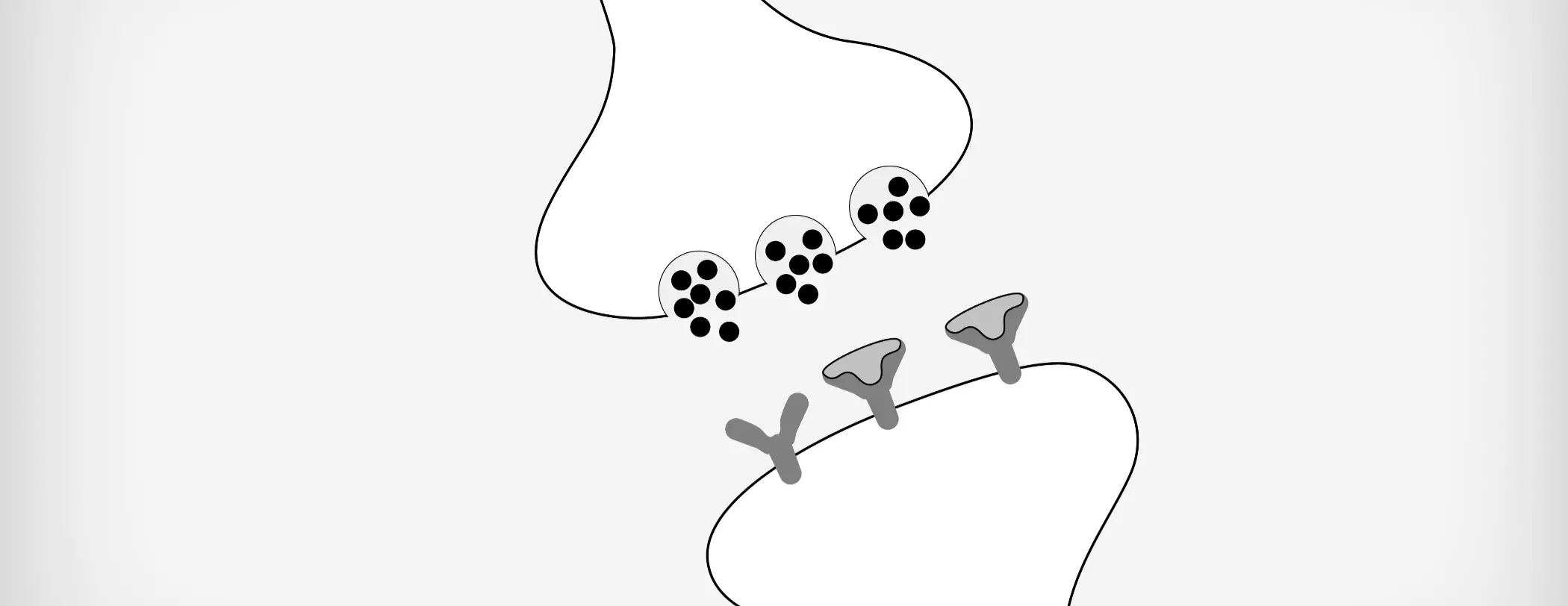
Normally, movement is controlled by dopamine signaling in the basal ganglia.5 The presynaptic neuron receives a signal to initiate movement and a postsynaptic neuron transmits the signal to produce movement.4,5
Dopamine is present in the presynaptic neuron and is packaged into synaptic vesicles via vesicular monoamine transporter 2.4,5 When the signal to initiate movement is received by the presynaptic neuron, the vesicles fuse with the presynaptic membrane and release dopamine into the synapse.4,5 Dopamine then binds to dopamine D2 receptors on the postsynaptic neuron.4,5 Then a signal is transmitted to the postsynaptic neuron, ultimately resulting in movement.4,5
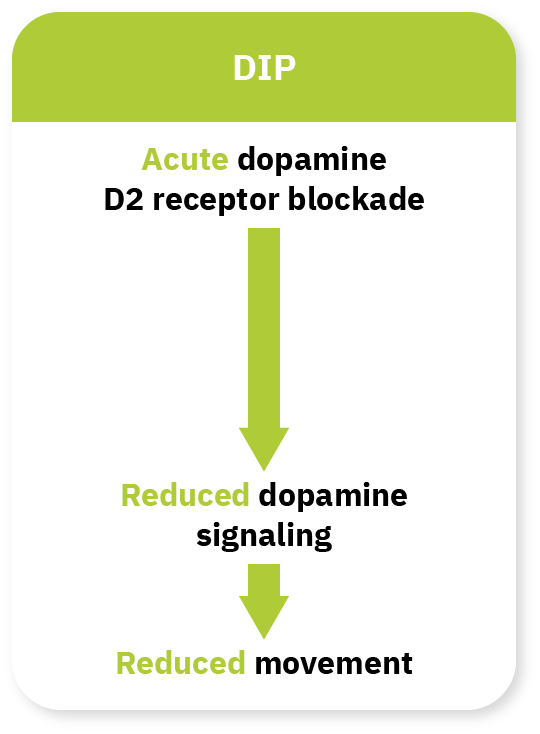
In DIP, the initiation or increase in the dose of an antipsychotic leads to the acute blockade of the dopamine receptors, which results in decreased dopamine signaling.4 Thus, when dopamine is released, the antipsychotic is bound to dopamine receptors, and the blockade results in reduced dopamine signaling in the postsynaptic neuron. Reduced dopamine signaling results in bradykinesia or slowness of movement.4
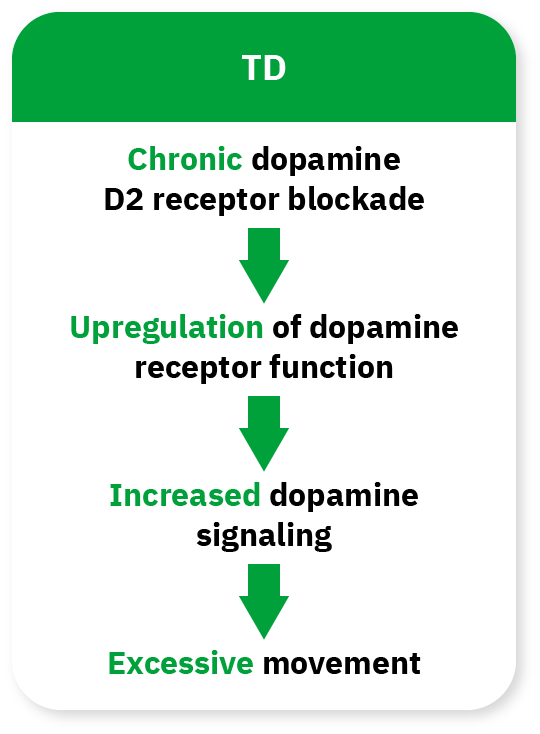
The exact pathophysiology of TD is not fully understood. However, it is thought that in TD, chronic blockade of dopamine receptors by the antipsychotic results in the upregulation of dopamine receptor function, possibly due to hypersensitivity or an increase in the number of dopamine receptors. This results in increased dopamine signaling, which manifests as the excessive movements characteristic of TD.1,4
In summation, although TD and DIP are both movement disorders associated with patients taking antipsychotic drugs, they occur due to opposing mechanisms within the dopaminergic pathway.1,2 In DIP, the blockade of dopamine reduces dopamine signaling, subsequently resulting in hypokinetic movement such as bradykinesia (Figure 1).4 In TD, there is upregulation of dopamine receptors, resulting in increased dopamine signaling, which manifests as hyperkinetic movement.1,4
Given these differing etiologies, the differing symptoms of each disorder, and the implications of misdiagnosis, it is important to base treatment decisions on accurate diagnosis of TD and DIP.1,4




