
Tardive dyskinesia (TD) and drug-induced parkinsonism (DIP) are common movement disorders caused by exposure to antipsychotic drugs (APDs).1,2 TD or DIP present in as many as 1 of 3 patients taking antipsychotics.1,2 Historically, TD and DIP were both considered to be “extrapyramidal symptoms” (EPS).3-5 However, TD and DIP are distinct conditions with different treatment approaches.3 The choice of therapy should be thoughtfully made based on the diagnosis, as the treatment for one disorder may worsen the other.2,3 A significant number of patients with TD are prescribed an anticholinergic, such as benztropine, even though these agents can exacerbate TD symptoms.2,6,7 Recognizing and subscribing to the American Psychiatric Association (APA) and Diagnostic and Statistical Manual of Mental Disorders, 5th Edition, Text Revision (DSM-5-TR) recommendations for both TD and DIP may help delineate the important distinctions among the 2 disorders and guide clinicians on how best to approach treatment.6,8
TD is underdiagnosed or misdiagnosed, and patients who are diagnosed with TD are often inappropriately prescribed anticholinergics.7,9 In the United States, TD affects approximately 785,000 patients; about 15% of patients with TD receive a formal diagnosis, and less than 6% of patients are treated with vesicular monoamine transporter 2 (VMAT2) inhibitors.9 This treatment gap may be due to the use of incorrect treatments for TD.7 In fact, according to Chepke and colleagues, approximately 40% of psychiatry providers would initiate benztropine to treat TD.7 In a longitudinal analysis looking at patients with TD over a 6-year period, ~36% are receiving an anticholinergic, such as benztropine. In an additional analysis of patients with TD, ~75% were treated with benztropine for >3 months, and ~35% of patients were treated for >1 year.
With fewer than 40% of psychiatry providers familiar with the 2020 APA practice guideline for the treatment of schizophrenia, the distinction between TD and DIP is generally misunderstood among the greater healthcare community.7 Recognizing and subscribing to the APA and DSM-5-TR recommendations for both TD and DIP may help delineate the important distinctions between the 2 disorders.6,8
For TD, the APA guidelines recommend that symptoms that have an impact on the patient, regardless of severity, should be managed with a VMAT2 inhibitor.8 According to the DSM-5-TR, the symptoms of TD tend to be worsened by anticholinergic medications, such as benztropine.6 Overall, both the APA guidelines and DSM-5-TR caution against using anticholinergics to treat TD.6,8
For DIP, anticholinergic medications such as benztropine are indicated for the treatment of DIP but not TD. However, there are consequences to consider when prescribing anticholinergic medications. The APA guidelines highlight the consequences of anticholinergic therapy for patients and state that “medications with anticholinergic effects can result in multiple difficulties for patients, including impaired quality of life, impaired cognition, and significant health complications.”8,10 The guidelines also recommend that anticholinergics should not be administered prophylactically. If anticholinergic therapy is needed, it should be used at the lowest dose for the shortest possible time.5,8
TD and DIP can be easily differentiated with a baseline understanding of the timing of onset and associated symptoms.11 DIP usually develops within a few weeks to months of starting or increasing the dosage of an APD or reducing the dosage of a medication used to treat EPS (eg, anticholinergic).2,6 On the other hand, symptoms of TD develop after using an APD for at least a few months to years.2,6 TD movements may appear after discontinuing or reducing the antipsychotic, whereas DIP will usually resolve when this occurs.6
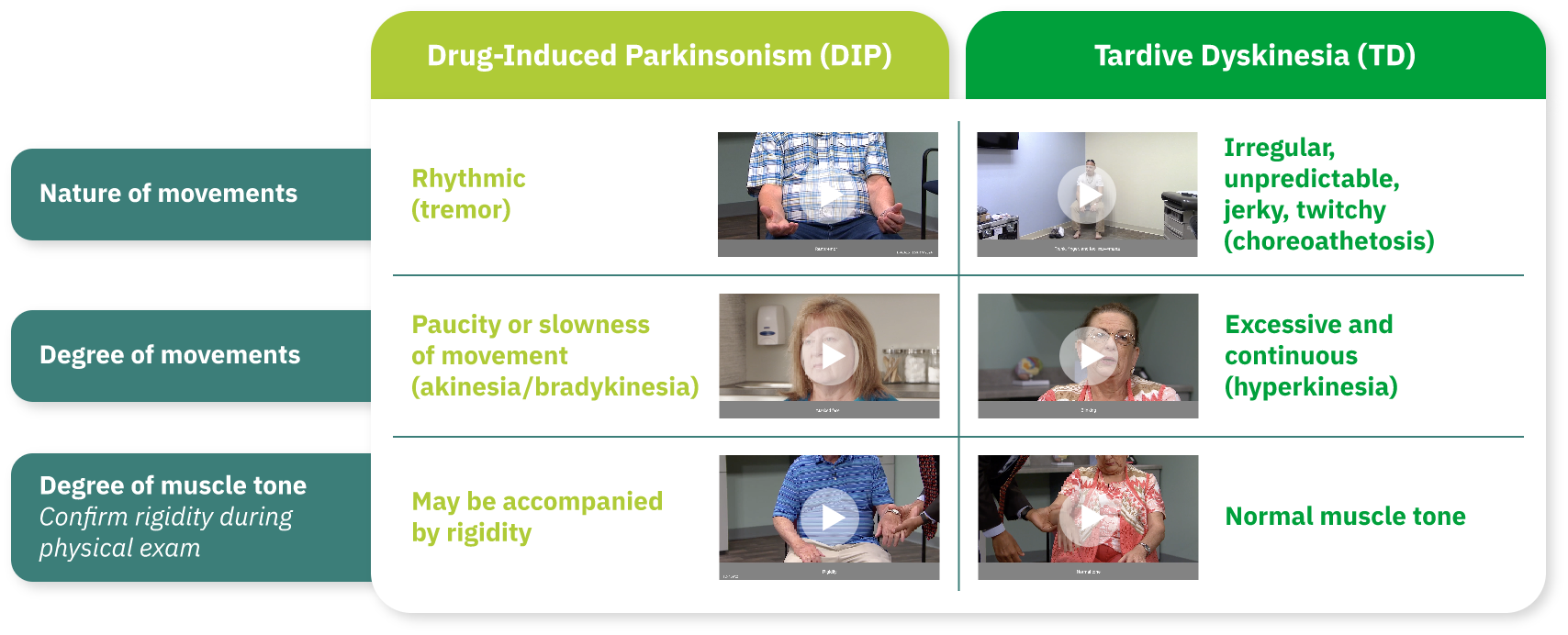
TD and DIP are associated with different types of movements (Figure 1).11 The key symptoms that differ between the 2 disorders include the nature and degree of movements.11 TD is characterized by an excess of movements that are irregular, jerky, and unpredictable and are accompanied by normal muscular tone.6,11 However, DIP is characterized by a paucity of movement. When movements occur, they are typically rhythmic, and patients with DIP may also exhibit muscle rigidity.11 It is important to note that DIP and TD may co-occur. Testing for parkinsonian rigidity is an important component of the Abnormal Involuntary Movement Scale (AIMS) examination because rigidity may partially or completely mask dyskinesia.12 It is also important to note that the AIMS can be used to identify DIP as well.
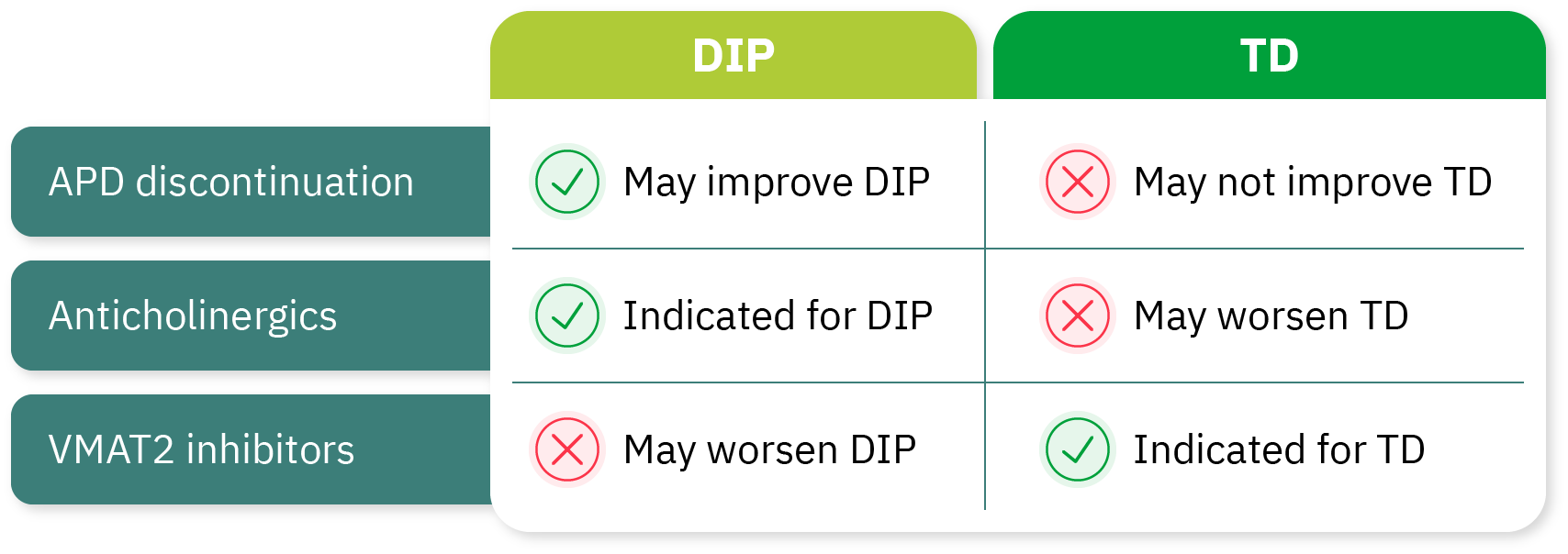
Once the provider is comfortable differentiating between TD and DIP, understanding the treatment choice becomes clearer. Due to the differences between TD and DIP, consideration must be given to which treatment approach can best address the specific condition.2,6 Discontinuing, reducing the dose, or changing to a different APD may improve or resolve the symptoms associated with DIP, while APD dose reduction or withdrawal may fail to improve the symptoms of TD and may even induce withdrawal dyskinesia.2,6,14 As noted, anticholinergics are indicated for the treatment of DIP but can worsen TD symptoms, whereas VMAT2 inhibitors are recommended for adults with TD but can worsen DIP symptoms (Figure 2).2,6,8
Although TD and DIP are common movement disorders caused by exposure to APDs, they are 2 distinct conditions with different treatment approaches.1-4 The choice of therapy should be thoughtfully made based on the diagnosis, as treatment for one disorder may worsen the other.2,3 Many patients with TD incorrectly receive anticholinergic treatments indicated for DIP, such as benztropine, which may worsen TD.10 Once HCPs proactively identify and diagnose TD and DIP, they must consider expert guidelines, such as the APA guidelines and DSM-5-TR recommendations, to make informed treatment decisions to optimize the opportunity to improve a patient's quality of life.6,8




