
All patients taking antipsychotic drugs (APD) are at a risk of developing tardive dyskinesia (TD), which can have a profound impact on many aspects of patients' lives, including psychological, social, physical, and vocational/educational effects.2-6 TD can also complicate the management of the underlying mental health disorder.7 The American Psychiatric Association (APA) guidelines recommend vesicular monoamine transport type 2 (VMAT2) inhibitors as first-line treatment for TD regardless of severity, as mild symptoms of TD can also have a substantial impact on day-to-day functioning and social functioning.1 In addition, VMAT2 inhibitors are recommended for TD without the requirement to modify the APD dose.1
Once-daily AUSTEDO XR is an extended-release VMAT2 inhibitor approved in adults for the treatment of TD.8 Bioequivalence of AUSTEDO XR has been established with AUSTEDO BID based on pharmacokinetic profile studies performed across 3 phase 1 clinical trials in healthy volunteers.9 In the bioequivalence study, peak plasma concentrations (Cmax) of AUSTEDO XR were reached within approximately 3 hours followed by a sustained plateau during the majority of the 24-hour dosing interval (Figure 3.1).9
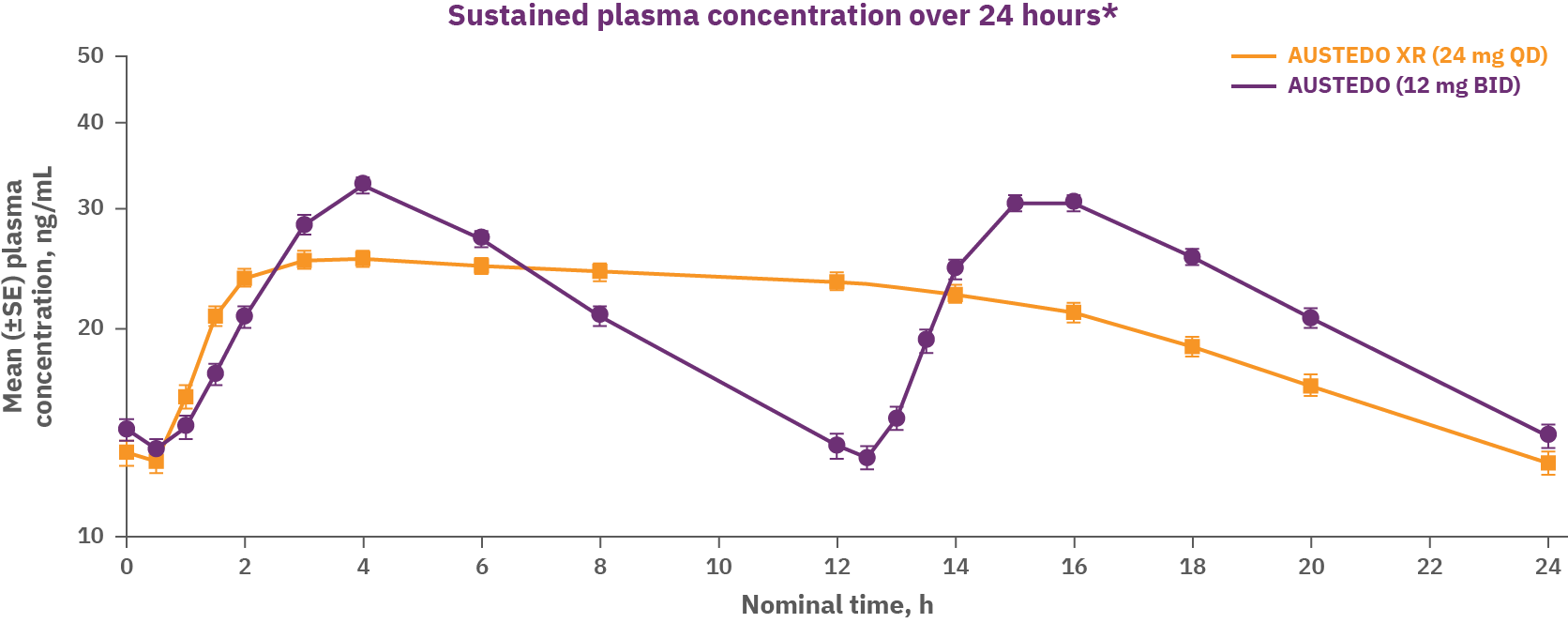
The US Food and Drug Administration (FDA) defines bioequivalence as the absence of a significant difference in the drug exposure profile of 2 drugs.10 When 2 formulations are shown to be bioequivalent, they can be considered therapeutically equivalent.10 Data support equivalence of AUSTEDO XR and AUSTEDO BID across the full clinical dosing range (12 mg QD to 48 mg QD).9
The ARM-TD, AIM-TD, and RIM-TD clinical trials were conducted to assess efficacy and safety of AUSTEDO in patients with TD. Patients in these clinical trials received the AUSTEDO BID formulation.11-13
ARM-TD was a flexible-dose clinical trial in which patients' doses were individually titrated to a level that was tolerated and reduced abnormal movements.8,11,12 Patients were randomized 1:1 to receive AUSTEDO or placebo. The starting dose of AUSTEDO was 12 mg/day, which was increased by 6 mg/day each week until satisfactory control of TD was achieved, until intolerable side effects occurred, or until a maximal dose of 48 mg/day was reached. Patients were titrated to an optimal dose over 6 weeks. The 12-week treatment period included this 6-week titration period and a 6-week maintenance period and was followed by a 1-week washout.8,12
The primary efficacy endpoint for this study was the change from baseline (defined for each patient as the value from the day 0 visit) to Week 12 in Abnormal Involuntary Movement Scale (AIMS) total score (sum of items 1 through 7) as assessed by 2 blinded central video ratings. Higher AIMS scores are indicative of more severe dyskinesia.8,9,12 Patients in the ARM-TD study showed a significant improvement in AIMS total score from baseline at Week 12 vs placebo (3.0-point reduction vs 1.6-point reduction; P=0.019).9
AIM-TD was a 12-week, randomized, double-blind, placebo-controlled, fixed-dose trial in which patients were randomized 1:1:1:1 to placebo or AUSTEDO 12 mg, 24 mg, or 36 mg. Treatment duration included a 4-week dose-escalation period and an 8-week maintenance period followed by a 1-week washout. The dose of AUSTEDO was started at 12 mg/day and increased at weekly intervals in 6-mg/day increments to a dose target of 12, 24, or 36 mg/day.8,11 The primary efficacy endpoint was change from baseline to Week 12 in AIMS total score in the 36-mg/day group vs placebo, assessed by blinded central video rating. In AIM-TD, AUSTEDO significantly reduced AIMS total score by 3.3 points from baseline in the 36-mg/day arm (vs a reduction of 1.4 points with placebo) at Week 12 (P=0.001, treatment effect of -1.9 points).8,9,11 In an exploratory analysis, significant AIMS total score reduction was seen at 2 weeks for the 24- and 36-mg/day groups.11
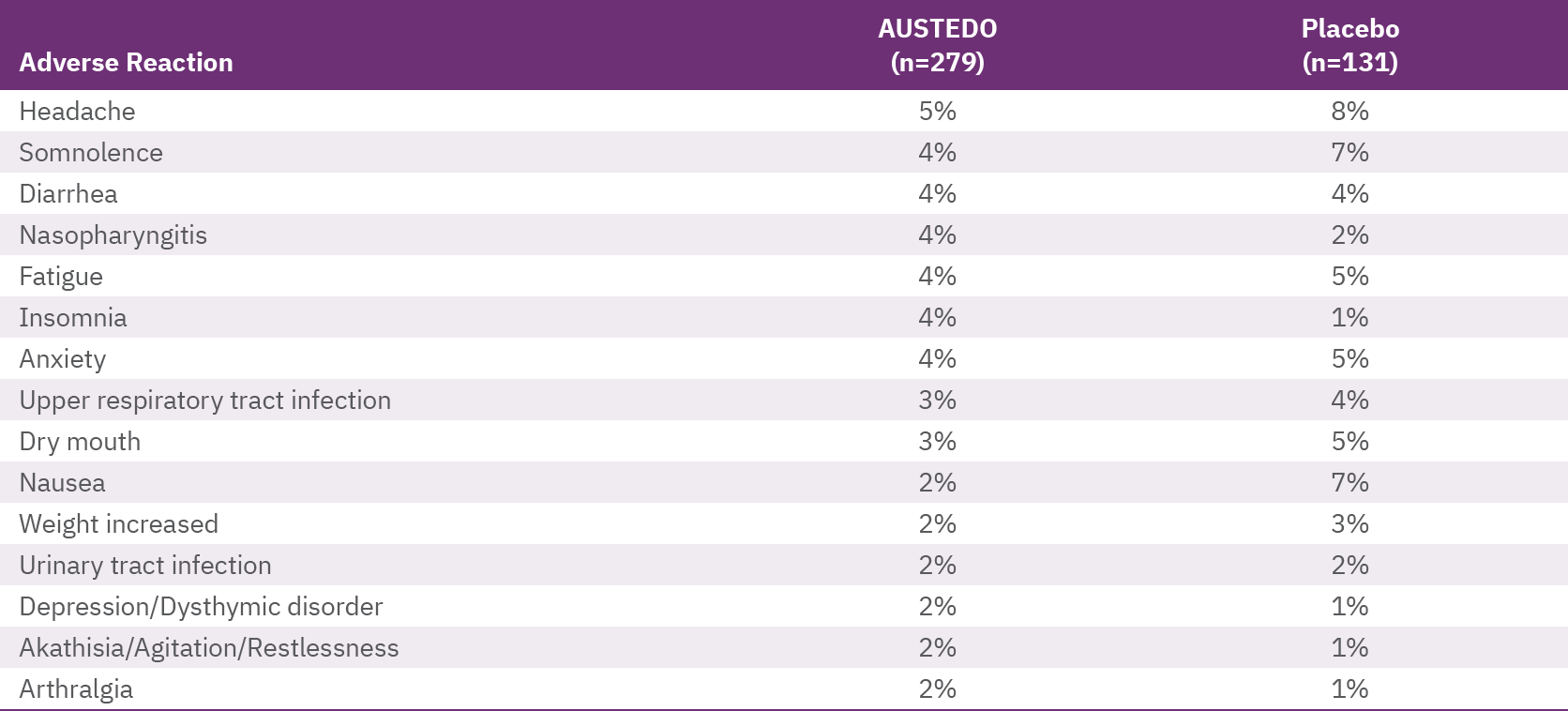
The most commonly reported adverse effects by patients treated with AUSTEDO (3% and greater than placebo) in the placebo-controlled studies were nasopharyngitis and insomnia (Table 3.1).8 Discontinuation due to adverse reactions occurred in 4% of patients taking AUSTEDO vs 3% of patients taking placebo.11 Dose reduction due to adverse reactions was required in 4% of patients taking AUSTEDO vs 2% of patients taking placebo.8 Adverse reactions with AUSTEDO XR are expected to be similar to AUSTEDO BID.8 The safety profile from the RIM-TD 3-year study was comparable to the safety profiles from the 12-week clinical trials.13 There were no new safety signals identified in RIM-TD.13
RIM-TD was an open-label, long-term maintenance study in patients who successfully completed ARM-TD or AIM-TD. Patients discontinued AUSTEDO for 1 week and then started at a dose of 12 mg/day, which was titrated for up to 6 weeks. The dose was increased in a response-driven manner on a weekly basis by 6 mg/day until either the maximum allowable dose was reached, a clinically significant adverse event (AE) occurred, or adequate dyskinesia control was achieved. Patients were followed for approximately 3 years (145 weeks).13
Among the patients evaluated, 337 patients had treatment at baseline and 160 patients had treatment through the end of Week 145. During the overall treatment period, patients generally experienced an improvement in the AIMS total score. There was a gradual reduction in the mean AIMS total scores from baseline through Week 145 (Figure 3.2).13 The average dose of AUSTEDO was >36 mg/day (39.4 mg/day at Week 145).13
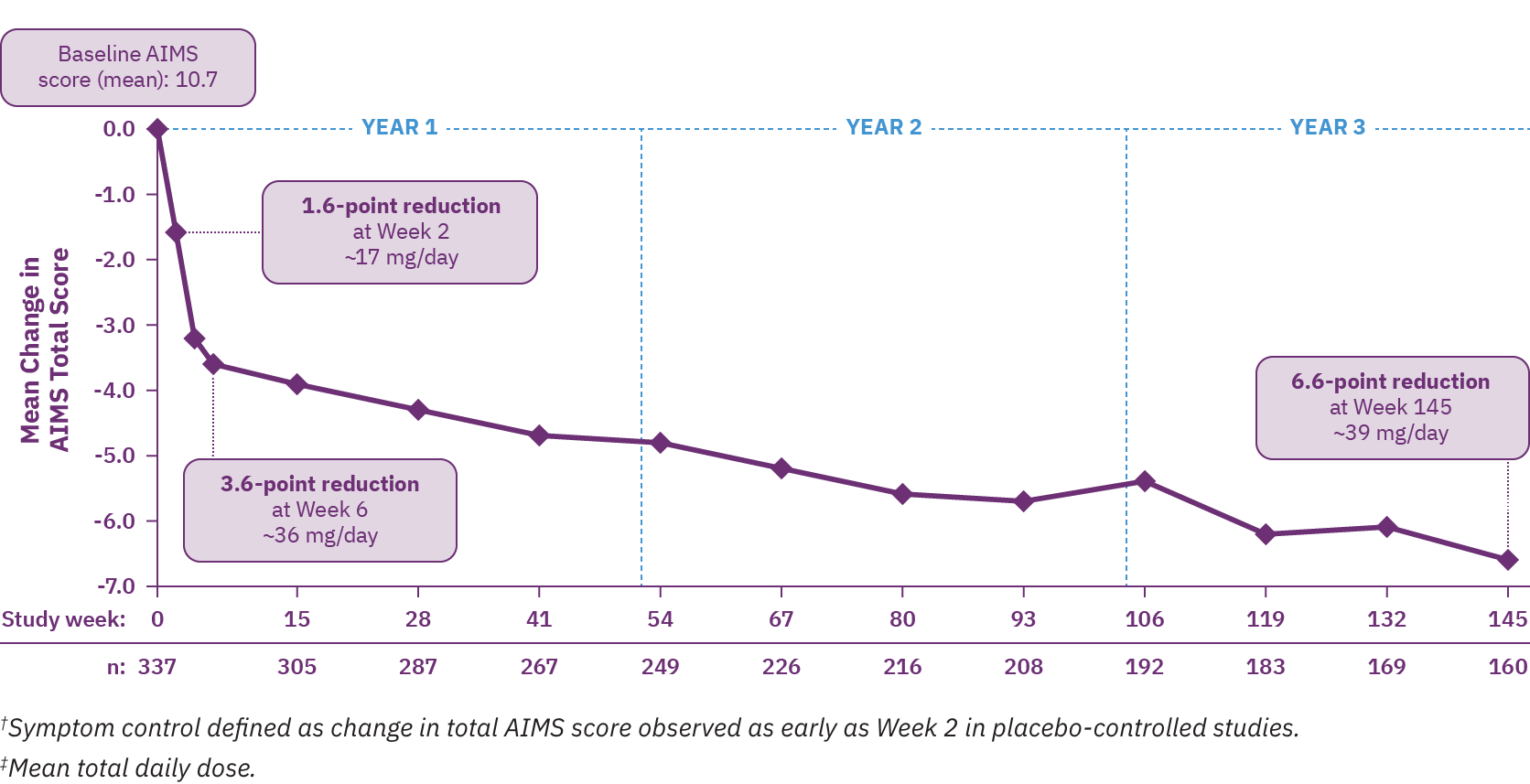
At Week 145 in RIM-TD, 67% of patients achieved ≥50% improvement in AIMS total score.13 Clinicians and patients generally recognized improvement in TD symptoms with AUSTEDO treatment based on assessments of Clinical Global Impression of Change (CGIC) and Patient Global Impression of Change (PGIC) over time. At Week 145, a majority of patients (63%) and physicians (73%) reported symptoms as “much improved” or “very much improved.”13 Preexisting psychiatric scores remained stable throughout the treatment period and AEs were comparable to those seen in the pivotal clinical trials.9,13 The mean overall compliance rate was nearly 90% at 3 years.9
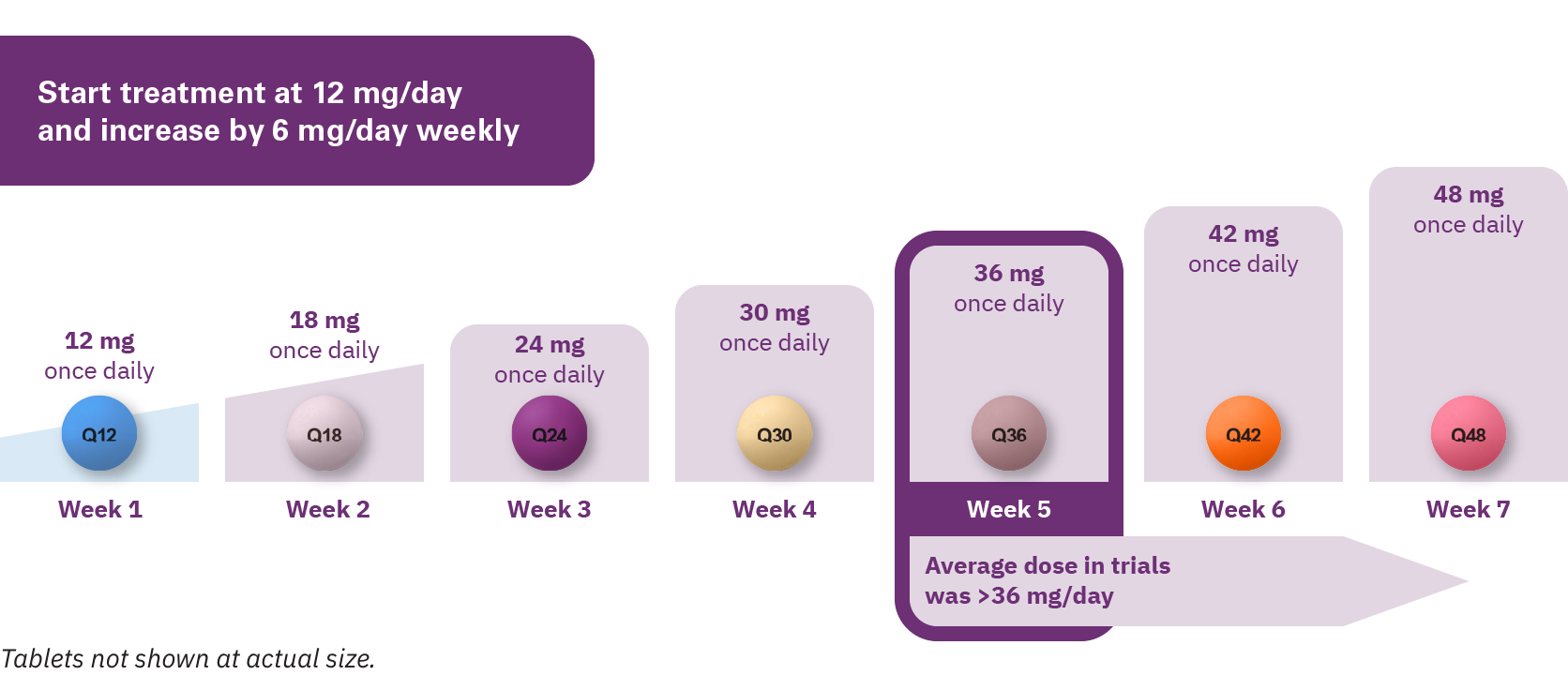
AUSTEDO XR is available in 12 mg, 18 mg, 24 mg, 30 mg, 36 mg, 42 mg, and 48 mg extended release tablets, providing flexibility for effective and tolerable symptom control.8
The recommended starting dose of AUSTEDO XR for patients with TD is 12 mg/day, which may be increased at weekly intervals by 6 mg/day until desired symptom control is tolerably achieved (Figure 3.3).8 The average daily dose in clinical trials was >36 mg/day.11-13 This average dose emphasizes the importance of titration, when appropriate, to help patients achieve desired symptom control.8,11-13 The maximum recommended daily dose of AUSTEDO XR is 48 mg/day.8
Once-daily AUSTEDO XR may be taken with or without food. AUSTEDO XR should be swallowed whole. Tablets should not be chewed, crushed, or broken.
To get new patients started on AUSTEDO XR, a 4-week Titration Kit is available through sample or prescription. For continuing patients, write once-daily AUSTEDO XR for the next refill at the same total daily dose as AUSTEDO BID.9
To summarize, the APA guidelines recommend VMAT2 inhibitors as first-line treatment for TD.1 Once-daily AUSTEDO XR is an extended-release VMAT2 inhibitor approved in adults for the treatment of TD.8 The bioequivalence of AUSTEDO XR has been established with AUSTEDO BID based on pharmacokinetic profile studies performed across 3 phase 1 clinical trials in healthy volunteers.9 The efficacy and safety of AUSTEDO BID in patients with TD was demonstrated in 3 clinical trials (ARM-TD, AIM-TD, and RIM-TD).11-13 Adverse reactions with AUSTEDO XR are expected to be similar to AUSTEDO BID.8 In the RIM-TD study, patients exhibited sustained results through 3 years.13 AUSTEDO XR is available as one pill, once daily for all doses. The recommended starting dose of AUSTEDO XR for patients with TD is 12 mg/day and may be increased at weekly intervals by 6 mg/day until desired symptom control is tolerably achieved.8,9




