This case study reviews the clinical considerations required when selecting a treatment for tardive dyskinesia (TD) in a patient with potential drug-drug interactions (DDIs).
TD is a persistent, typically irreversible, hyperkinetic movement disorder resulting from chronic exposure to dopamine receptor blocking agents, including antipsychotic drugs (APDs). Any presentation of TD can have a profound impact on many aspects of patients' lives and undermine the stability of the underlying mental health disorder.
Patients taking APDs to treat mental health disorders may be on several other medications for managing comorbidities. Consequently, clinicians must consider the whole patient, including any concomitant medications they may be on when choosing an appropriate therapy for TD.
This case study features Chris, a 55-year-old man currently taking extended-release carbamazepine for bipolar disorder and a glucocorticoid to manage rheumatoid arthritis. Owing to previous exposure to atypical APDs, he developed TD. He was prescribed AUSTEDO XR, as it is the only vesicular monoamine transporter 2 (VMAT2) inhibitor approved for TD with no recommendations against concomitant use with CYP3A4/5 inducers or inhibitors. This case study highlights the importance of reviewing patients' concomitant medications to avoid potential DDIs when choosing a therapy for TD.
Below, we detail this patient's medical history, TD diagnosis, treatment strategies, and decisions.

Not an actual patient
Chris is employed as a stockbroker and is twice divorced. He is currently taking extended-release carbamazepine to manage bipolar disorder after previous treatment with lithium and atypical APDs failed to stabilize his mental health condition. He also takes a glucocorticoid to manage his rheumatoid arthritis.
At the time of presentation, Chris complained of twitching in his fingers, jaw clenching, and excessive blinking due to dry eyes. The movements have caused him to be distracted at work, and he has had trouble staying focused on his stock trades. Additionally, his colleagues have commented that he appears anxious and restless.
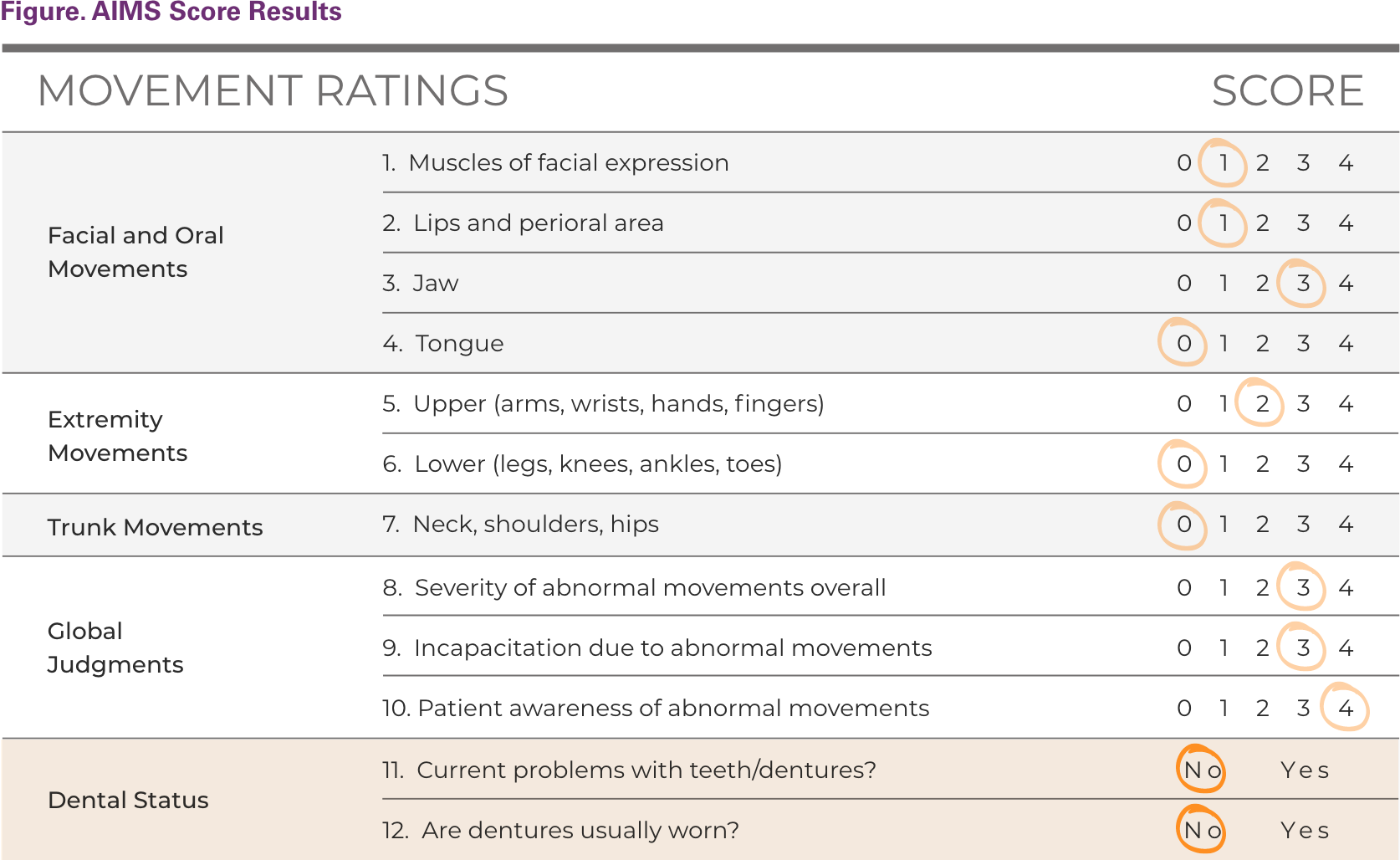
Recognizing that Chris had previous exposure to APDs, which increased his risk of TD, Chris’s psychiatrist performed an Abnormal Involuntary Movement Scale (AIMS) examination. Chris had movements scored as at least 2 on the AIMS and affecting at least 1 body part. The sum of his movement scores resulted in a total AIMS score of 7 (Figure). The clinician reported that the movements were choreoathetoid in nature and primarily affected the orofacial region.
The American Psychiatric Association (APA) recommends treatment with a VMAT2 inhibitor for TD that has an impact on the patient, as is the case with Chris.
An important consideration for Chris is that his medication regimen cannot be modified because previous treatment with lithium and atypical APDs failed to effectively manage his bipolar disorder. He is currently stable on carbamazepine extended release and is taking a glucocorticoid, which are both strong CYP3A4 inducers. When reviewing treatment options for Chris's TD, his current medications should be reviewed for potential DDIs.
What did Chris's psychiatrist decide to prescribe and why?
Chris's psychiatrist decided to prescribe AUSTEDO XR, which is indicated for adults with TD based on bioequivalence with the AUSTEDO twice-daily formulation, for which safety and efficacy were established in 2 phase 3, randomized, placebo-controlled clinical trials.
The most common adverse reactions occurring in greater than 3% of AUSTEDO-treated patients and greater than placebo were nasopharyngitis and insomnia. Adverse reactions with AUSTEDO XR extended-release tablets are expected to be similar to AUSTEDO tablets.
AUSTEDO XR was also chosen because Chris is taking extended-release carbamazepine, a strong CYP3A4 inducer, and AUSTEDO XR is the only VMAT2 inhibitor indicated for TD with no dose restrictions for, or recommendations against, use in patients taking strong CYP3A4/5 inducers or inhibitors.
Chris was provided a 4-week Titration Kit of AUSTEDO XR, instructed to call the office in 2 weeks to check in, and asked to schedule a follow-up visit in 4 weeks.
What was the result of Chris's treatment?
After 2 weeks on once-daily AUSTEDO XR, Chris called the office and reported that he had noticeable improvements in his jaw clenching and finger movements.
At his 4-week follow-up appointment, his AIMS score was reduced from 7 to 4. Chris's eye blinking persisted, and he was referred to a rheumatologist for further evaluation of his dry eyes because they could be a symptom of rheumatoid arthritis.
Chris was instructed to schedule another follow-up visit in 4 weeks.
Chris's symptoms were a red flag for his psychiatrist, who recognized he was at risk for TD. Based on the results of the AIMS, the DSM-5-TR criteria for TD, and expert consensus for diagnosis of TD, Chris's provider diagnosed Chris with TD.
The APA recommends that patients who have moderate to severe or disabling TD associated with antipsychotic therapy be treated with a reversible inhibitor of VMAT2. APA guidelines recommend considering a VMAT2 inhibitor to address TD-associated impairments and impact on social functioning.
An important factor psychiatrists must consider when choosing a treatment for TD is the potential for DDI. Chris was taking extended-release carbamazepine and glucocorticoid, which are both strong CYP3A4 inducers. As a result, his clinician had to select a treatment option for TD with no induction of CYP3A4.
Chris's provider selected AUSTEDO XR because it is the only VMAT2 inhibitor indicated for TD with no recommendations against concomitant use with CYP3A4/5 inducers or inhibitors.
Chris reported noticeable improvements in jaw clenching and finger movements after completing the 4-week Titration Kit of AUSTEDO XR, although eye blinking persisted, and he was referred to a rheumatologist for further evaluation.
Adverse reactions with AUSTEDO XR are expected to be similar to AUSTEDO BID.
Chris's case illustrates why psychiatry providers should consider metabolic pathways when choosing a treatment for patients with TD with potential DDIs.
Abd-Allah NM, Hassan AA, Omar G, et al. Dry eye in rheumatoid arthritis: relation to disease activity. Immunol Med. 2020;43(2):92-97.
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed, Text Revision. Washington, DC: American Psychiatric Association; 2022.
Anderson KE, Stamler D, Davis MD, et al. Deutetrabenazine for treatment of involuntary movements in patients with tardive dyskinesia (AIM-TD): a double-blind, randomised, placebo-controlled, phase 3 trial. Lancet Psychiatry. 2017;4(8):595-604.
Caroff SN, Citrome L, Meyer J, et al. A modified Delphi consensus study of the screening, diagnosis, and treatment of tardive dyskinesia. J Clin Psychiatry. 2020;81(2):19cs12983.
Caroff SN, Yeomans K, Lenderking WR, et al. RE-KINECT: a prospective study of the presence and healthcare burden of tardive dyskinesia in clinical practice settings. J Clin Psychopharmacol. 2020;40(3):259-268.
Fahn S, Jankovic J, Hallet M, eds. Principles and Practice of Movement Disorders. 2nd ed. Amsterdam, The Netherlands: Elsevier, Inc; 2011.
Fernandez HH, Factor SA, Hauser RA, et al. Randomized controlled trial of deutetrabenazine for tardive dyskinesia: the ARM-TD study. Neurology. 2017;88(21):2003-2010.
Hauser RA, Meyer JM, Factor SA, et al. Differentiating tardive dyskinesia: a video-based review of antipsychotic-induced movement disorders in clinical practice. CNS Spectr. 2022;27(2):208-217.
Horn JR, Hansten PD. Get to know an enzyme: CYP3A4. Pharmacy Times. September 1, 2008. Accessed February 5, 2024. https://www.pharmacytimes.com/view/2008-09-8687
Jain R, Ayyagari R, Goldschmidt D, Zhou M, Finkbeiner S, Leo S. Impact of Tardive Dyskinesia on Physical, Psychological, Social, and Professional Domains of Patient Lives: A Survey of Patients in the United States. J Clin Psychiatry. 2023;84(3):22m14694.
Zutshi D, Cloud LJ, Factor SA. Tardive syndromes are rarely reversible after discontinuing dopamine receptor blocking agents: experience from a university-based movement disorder clinic. Tremor Other Hyperkinet Mov (N Y). 2014;4:266.





