
An estimated 43 million people in the United States suffer from schizophrenia and mood disorders, including bipolar disorder and depression, for which antipsychotic drugs (APDs) are widely prescribed.1-7 Since their first approval in 1989 for schizophrenia, atypical APDs have been prescribed to an increasing number of patients due to the expansion of the indication to treat bipolar disorder (first approval in 2000) and depression (first approval in 2007).8-12 From 2017 to 2022, the number of patients treated with APDs increased by 22%, a rise primarily driven by atypical APD prescriptions.13
While APDs are critical in helping to maintain the stability of patients’ mental health, their use carries the risk of developing tardive dyskinesia (TD), a persistent hyperkinetic movement disorder resulting from chronic exposure to APDs and other dopamine receptor blocking agents, including antiemetic agents.14-16 In a meta-analysis that examined the prevalence of TD in patients being treated with APDs, approximately 1 in 3 patients treated with typical APDs and up to 1 in 5 patients treated with atypical APDs had developed TD.17,* TD is characterized by typically irreversible involuntary movements that most often affect the orofacial region but can affect the whole body.14,16
In the United States, TD affects approximately 785,000 patients; however, TD may be underdiagnosed and undertreated. It has been estimated that approximately 15% of patients with TD have received a formal diagnosis and less than 6% of patients have received appropriate treatment.13 Vesicular monoamine transporter 2 (VMAT2) inhibitors, are recommended for the treatment of moderate to severe or disabling TD and should be considered for the treatment of TD if it has an impact on the patient.18
Factors that increase the risk of TD include long-term exposure to APDs (particularly at higher doses), prior development of drug-induced parkinsonism (DIP), treatment of DIP with anticholinergics, mood disorder, substance use disorder, age (older than 55 years), and female sex (especially those who are postmenopausal).18-20 In a recent online survey of 269 patients with TD, 3 out of 4 patients reported that the impact of TD was severe.21,† TD can have a profound impact on many aspects of patients’ lives, with patients reporting impact across 4 key domains: social withdrawal, inability to perform work responsibilities, deterioration of physical independence, and worsening of psychiatric symptoms.21-24
TD can also complicate the management of the underlying mental health disorder.21,25 48% reported that they skipped doses of an antipsychotic medication or took less than the doctor instructed because of TD, 39% reported that they stopped taking antipsychotic medication altogether, and 36% stopped going to the doctor treating their underlying condition, which would be expected to worsen symptoms of the underlying psychiatric illness and potentially lead to relapse.21 American Psychiatric Association (APA) guidelines recommend treatment if TD, irrespective of severity, has an impact on the patient.18
Compared with the general population, patients with mental health disorders have a greater incidence of morbidity and premature mortality driven by a higher prevalence of risk factors associated with cardiovascular disease.26 These risk factors can be further exacerbated by treatment with APDs, which carry a significant risk of weight gain, metabolic syndrome (dyslipidemia, hypertriglyceridemia, glucose dysregulation, diabetes), and hyperprolactinemia.7,26
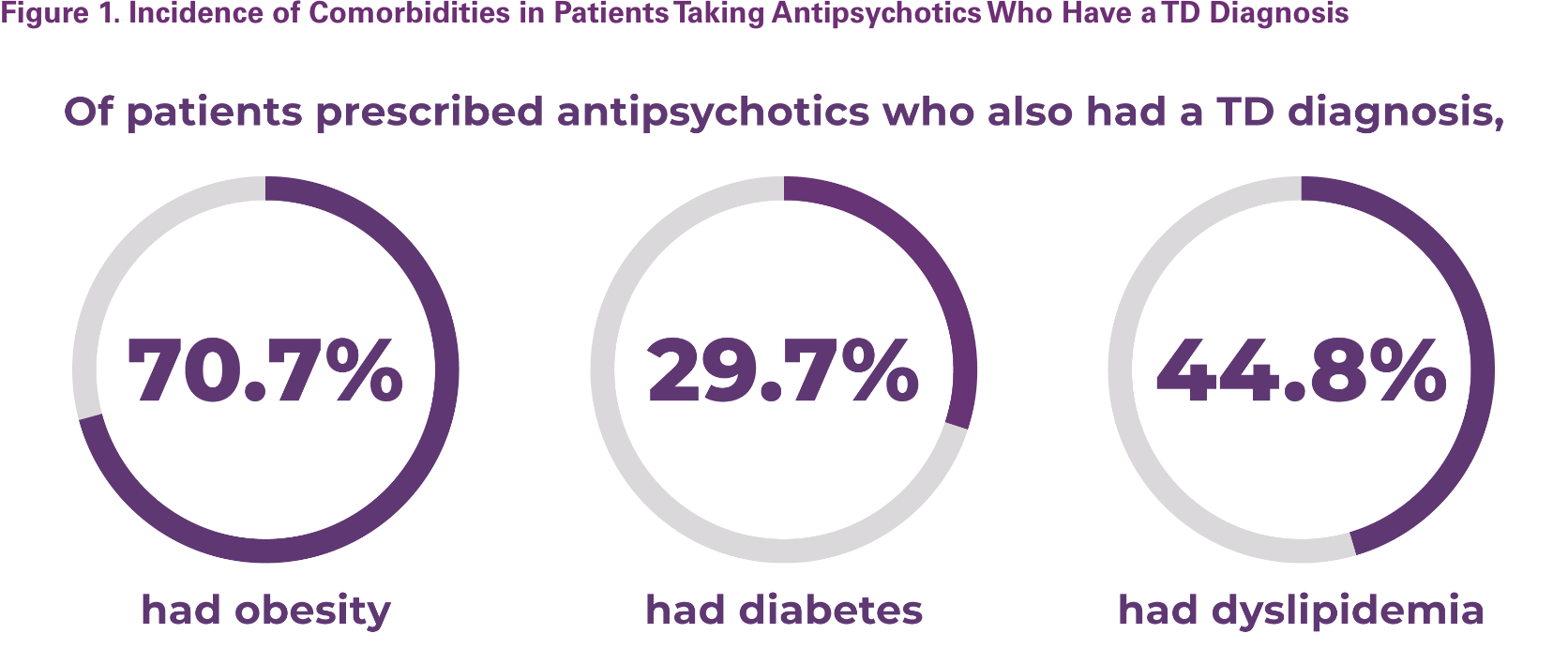
In a retrospective analysis using electronic health records, patients prescribed APDs demonstrated a high incidence of obesity, diabetes, and dyslipidemia, and these comorbidities were more prevalent in the TD population than in the entire APD cohort (Figure 1). APD-induced development of metabolic syndrome can be managed by switching to another APD with a different adverse effect profile or addition of adjunctive treatments that attenuate weight gain.27,28 A chart review of patients receiving medical management for their mental health disorders (MHDs) demonstrated that approximately half of medications taken were for nonpsychiatric comorbidities and that associated comorbid cardiometabolic disease significantly increased the total number of concomitant medication use, both psychiatric and nonpsychiatric.29
Other concomitant add-on medications that have gained wide acceptance for management of treatment-resistant agitation and aggression in patients with schizophrenia include benzodiazepines, antidepressants, antiparkinsonism drugs, mood stabilizers, and beta-adrenergic blockers.30 Patients treated for MHDs may receive 3 to 6 psychiatric and nonpsychiatric medications. In addition, use of APDs for management of MHDs is associated with the greatest rate of complex polypharmacy, defined as ≥ 4 concomitant medications.
As a result, polypharmacy is especially prevalent in patients taking APDs and is associated with several considerations, including the increased risk of drug-drug interactions (DDIs), adverse events, medication error, patient nonadherence, and medical comorbidities.29,31 To help reduce the risk of DDIs, treatment considerations for TD must take into account patients’ concomitant medications.
DDIs may occur when 2 or more drugs have synergistic or antagonistic pharmacodynamic effects, which may have a negative impact on patient and treatment outcomes.32 Overall, approximately 20% to 30% of adverse reactions are the result of DDIs, and the risk of DDIs increases to about 84% when the number of concomitant drugs rises from 2 to 6 agents.32 In addition, therapeutic efficacy is dependent on drug concentrations at the site of action, which is regulated by absorption, distribution, metabolism, and elimination.32 Therefore, identifying the metabolic pathways of each medicine that a patient is taking is essential to minimize DDIs.32
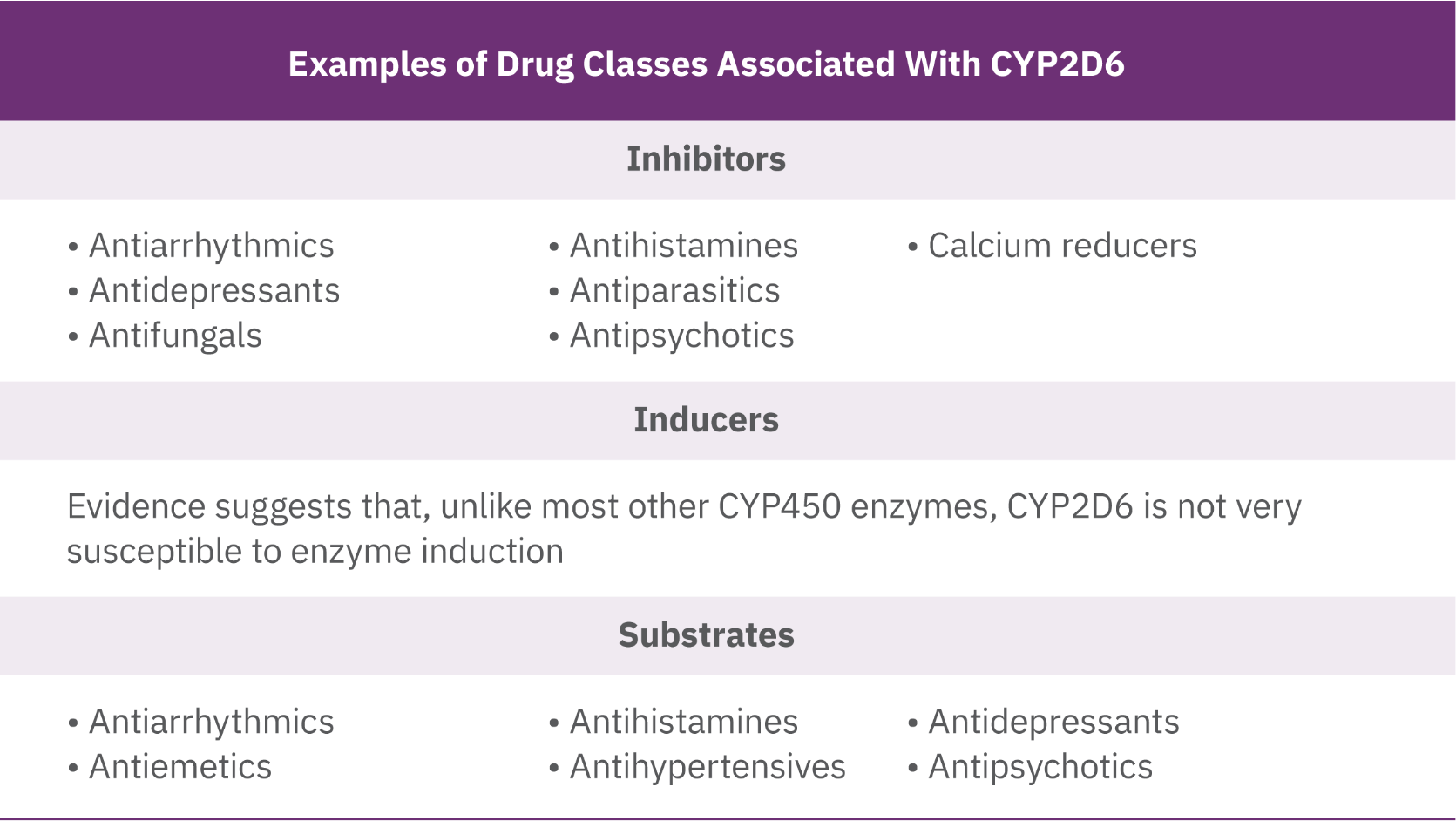
Drugs that serve as substrates, inhibitors, or inducers can have pharmacokinetic interactions with other medications, as well as with foods, beverages, and herbal supplements.32 When drug substrates are metabolized through the CYP450 pathway, CYP inducers cause increased enzyme activity, resulting in reduced drug activity.33 Conversely, CYP inhibitors simultaneously block activity, causing increased plasma levels of drugs or other substrates, which increases the risk of adverse effects, thereby requiring dosage reductions of medications.33 CYP3A4 and CYP2D6 are the most common metabolic pathways within the CYP450 enzyme family.34 About 80% of all approved drugs are metabolized through the CYP3A4 or CYP2D6 pathways—50% are metabolized through CYP3A4, and 30% through CYP2D6 (Table 1, Table 2).34
P-glycoprotein (P-gp) is another important protein in metabolism of ATPs not specific to the CYP450 pathway. P-gp resides in the intestinal epithelium and regulates drug absorption.32 P-gp is also found in liver cells, in the cells of proximal renal tubules, and in the capillaries of the blood-brain barrier. 32 Frequently, P-gp substrates, inhibitors, and inducers are also involved with the CYP450 system, making it challenging to isolate the specific pathway that caused the drug interaction.32
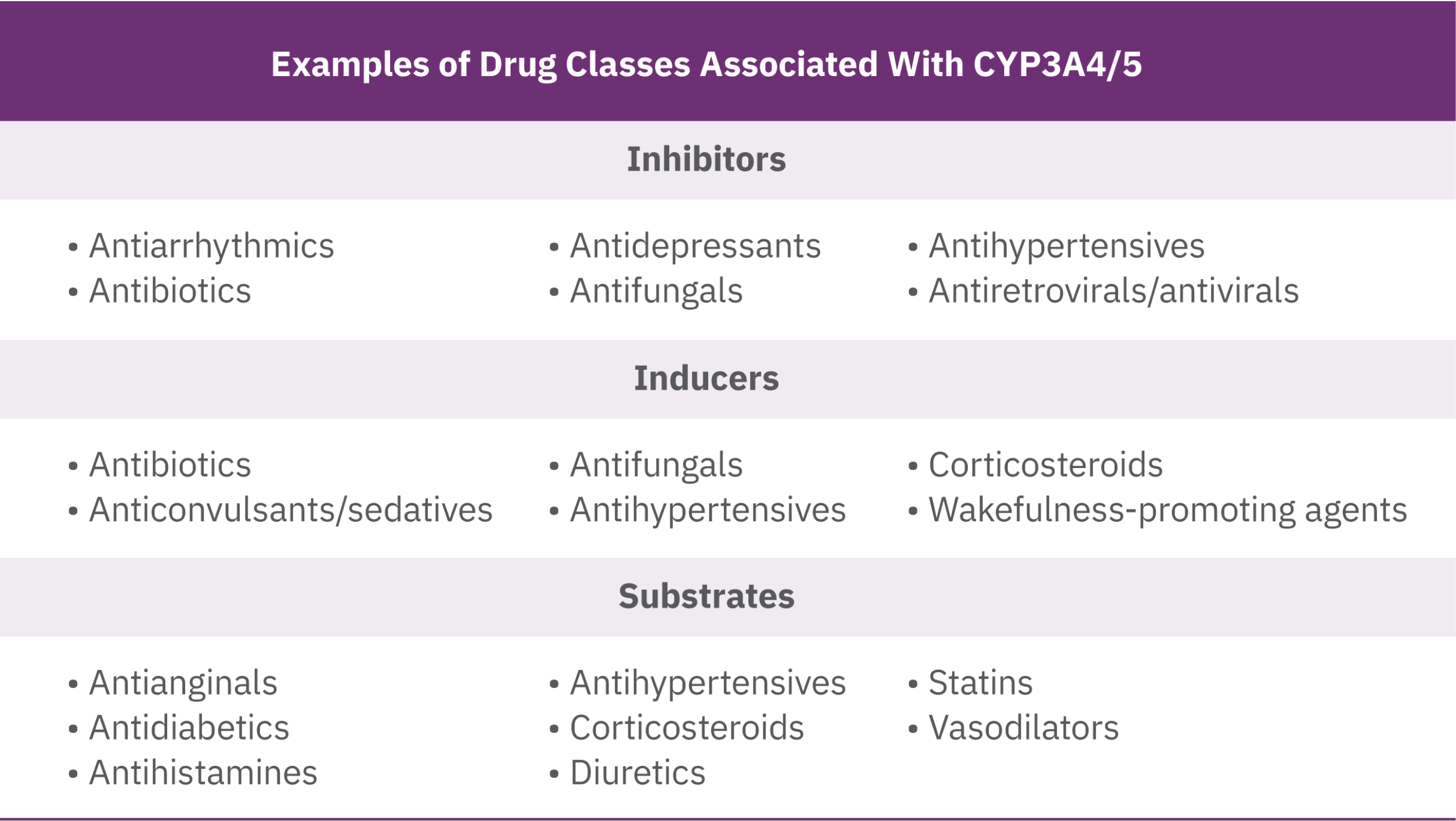
Potential DDIs can occur when patients receive treatment for mental health disorders and concomitant medications used to manage comorbidities.32 For example, many antihypertensives used to treat cardiovascular disease are substrates of the CYP3A4/5 pathway and may have their plasma levels modulated by inducers and inhibitors.32,35,36 Concomitant use of CYP3A4/5 inhibitors (eg, antibiotics) may increase the plasma levels of antihypertensives and increase the risk of falls and syncope.32 Similarly, inducers like anticonvulsants/sedatives may increase metabolism of antihypertensives, reducing therapeutic benefit (Table 1).13,32,35,36
Many psychotherapeutic medications, such as APDs and antidepressants, are inhibitors of the CYP2D6 pathway and can impact the metabolism of several CYP2D6 substrates used to treat chronic pain (opioids).32,36,37,38 In a study on opioids, concomitant administration with antidepressants (eg, selective serotonin reuptake inhibitors) showed the highest potential for DDIs due to modulating of plasma levels.38 In addition, some medications within the same class (eg, antipsychotics) can also induce arrhythmias if one is a substrate and the other an inhibitor of CYP2D6 (Table 2).13,32, 34,36,37
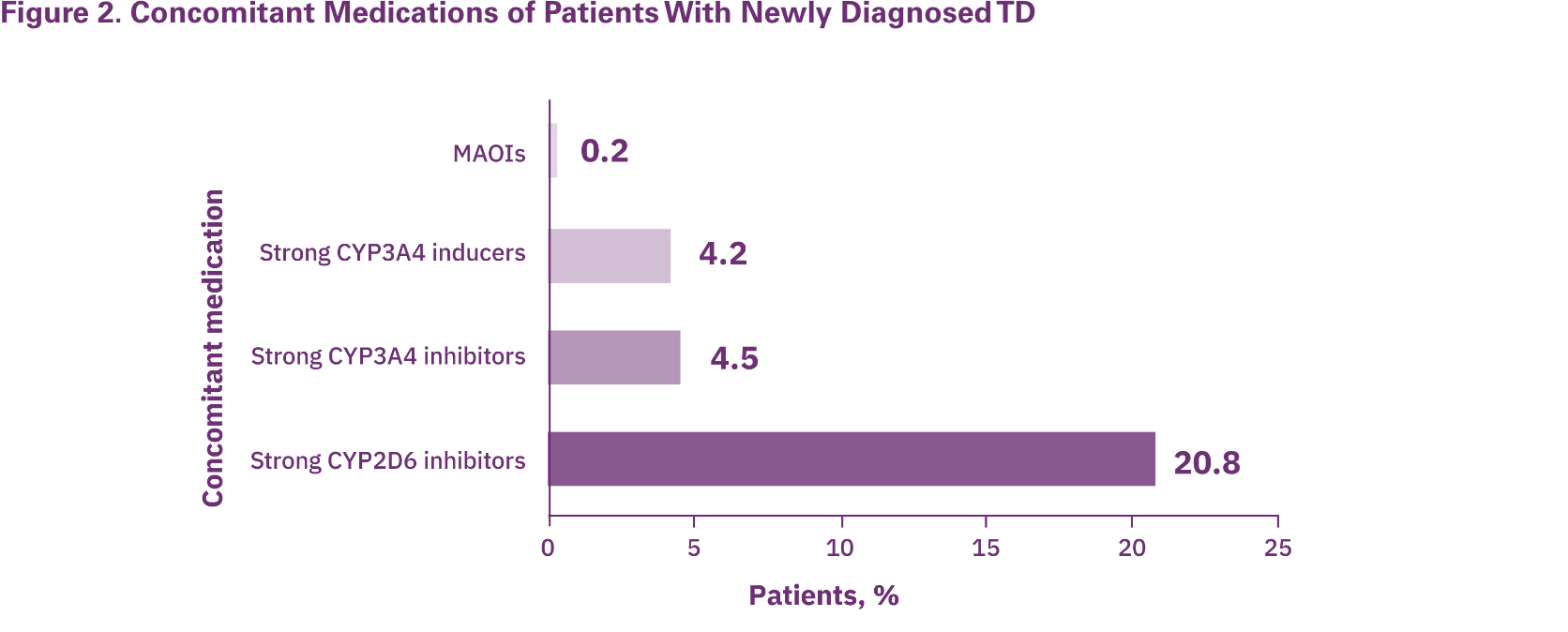
Managing TD in patients with comorbidities requires clinicians to be aware of all medications a patient is taking, as these can have important safety and therapeutic consequences.32 APA guidelines recommend VMAT2 inhibitors as first-line therapy for TD that impacts the patient.18 VMAT2 inhibitors currently approved for the treatment of TD should be reviewed for their potential DDIs with other medications that may act as strong inhibitors or inducers for the CYP3A4/5 and CYP2D6 pathways.39,40 A real-world study evaluating patients with newly diagnosed TD potentially at risk of DDIs with VMAT2 inhibitors, based on their concomitant medications at time of diagnosis, revealed that patients were taking strong CYP2D6 inhibitors, CYP3A4 inhibitors, CYP3A4 inducers, and monoamine oxidase inhibitors (MAOIs).41
When choosing a VMAT2 inhibitor, it is important to consider the patient's overall treatment plan and to identify drug metabolic pathways to reduce the risk for DDIs.39,40 For reference, consult the US Food and Drug Administration website that lists substrates, inducers, and inhibitors of both the CYP450 enzymes and transport proteins (https://www.fda.gov/drugs/drug-interactions-labeling/drug-development-and-drug-interactions-table-substrates-inhibitors-and-inducers#table5-1).
*As assessed in 28 global studies in the meta-analysis, approximately 1 in 14 patients treated with atypical APDs without previous exposure to a typical APD had TD.17
†From an online survey with one-time data collection from 269 patients with TD. 75.1% of patients reported severe impact (impact score of ≥4 on ≥1 item with each domain [physical, psychological, and social]), increasing from 61.5% for patients with no, mild, or moderate TD symptoms to 95.4% for patients with severe or very severe TD symptoms.21





