
This patient case study examines the assessment and diagnosis of tardive dyskinesia (TD), its impact on the patient's life, management of the patient's underlying mood disorder, and selection of an appropriate treatment.
Patients receiving treatment with dopamine receptor blocking agents, such as antipsychotic drugs (APDs), can develop TD, a persistent, typically irreversible hyperkinetic movement disorder. TD is characterized by involuntary, repetitive movements which most commonly affect the face, mouth, and tongue but can also manifest in the extremities and trunk. Although all patients receiving treatment with APDs are at risk for developing TD, those with mood disorders such as bipolar disorder and major depressive disorder are at increased risk. As APD use in this patient population continues to grow, clinicians must vigilantly screen for and assess symptoms of TD.
Compared to patients with schizophrenia, those with mood disorders generally have higher levels of cognition and can be severely impacted by even subtle TD movements. Any presentation of TD can have a consequential impact on a patient's life, yet healthcare professionals (HCPs) may not perceive the full extent of this. In fact, a survey indicated that 3 of 4 patients reported severe impact of TD on various domains of their lives. Additionally, the impact of TD has been shown to undermine the stability and management of a patient's underlying mental health disorder (Figure 1). Therefore, it is important for clinicians to inquire and uncover the impact of even subtle involuntary movements in all patients receiving treatment with APDs.
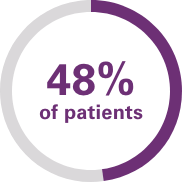
skipped doses of an antipsychotic medication or took less than the doctor instructed
skipped doses of an antipsychotic medication or took less than the doctor instructed
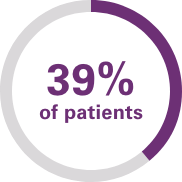
stopped going to the doctor treating their underlying condition

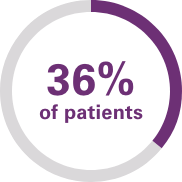
advised someone else not to take an antipsychotic medication
This case study features Laura, a 43-year-old woman who works full-time as a restaurant manager and is currently taking an atypical APD and lithium to manage bipolar depression. She is divorced and lives with her 23-year-old daughter, who recently was also diagnosed with bipolar depression and is managed with an atypical APD.

Not an actual patient
Laura was diagnosed with bipolar depression at age 22
At age 26, she was hospitalized for her first manic episode, after which she was treated with an atypical APD
At age 32, her clinician attempted to discontinue her atypical APD, which led to a second manic episode
Since then, she has been stable on an atypical APD and lithium
During an appointment with her clinician, Laura complains of clenching her teeth and blinking her eyes more than usual. While work has been going well, the restaurant has been busy, and she attributes these symptoms to increased stress. Due to the jaw pain from clenching her teeth and embarrassment from blinking, Laura has been canceling dates and is not going out with friends as much. Clinical examination shows excessive blinking, low-amplitude movement of the jaw, infrequent brow raising, and puckering of the perioral area.
For her jaw pain, Laura's clinician refers her to the dentist to be evaluated for temporomandibular joint disorder. He also recommends using lubricating eye drops, as he suspects that Laura's excessive blinking may be due to dry eyes.
Three months later, Laura returns to her clinician's office and continues to describe excessive blinking and pain from clenching her teeth. She shares that customers and colleagues are complaining to the restaurant owner that she is making unpleasant faces at them. She also notes that she has avoided meeting friends and family due to embarrassment.
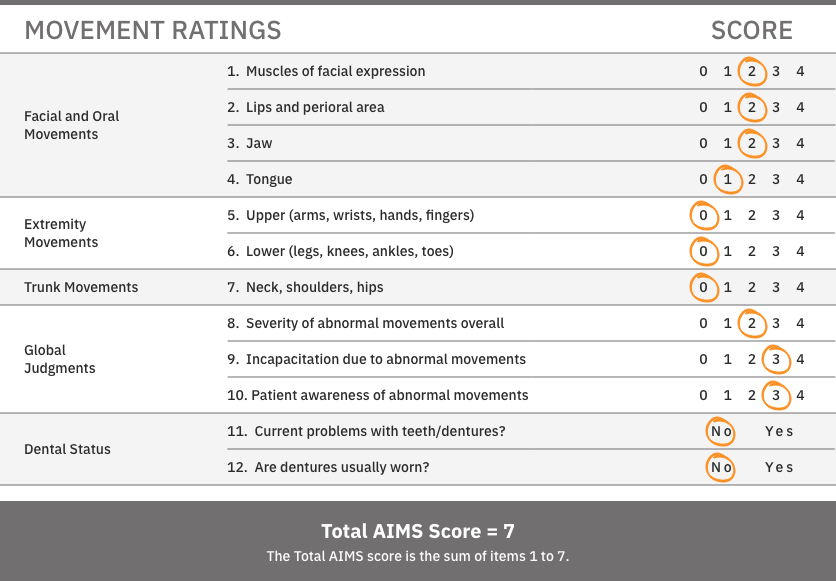
During this visit, the clinician carefully listens to Laura's concerns, notes the impact her symptoms are having, and takes a closer look at her facial movements. The clinician suspects TD and performs an Abnormal Involuntary Movement Scale (AIMS) examination, a structured assessment widely used to screen for and monitor TD symptoms, and reports a total AIMS score of 7 (Figure 2). Her clinician confirms the diagnosis of TD based on the DSM-5-TR criteria and a visual assessment.
Vesicular monoamine transporter 2 (VMAT2) inhibitors are recommended by the American Psychiatric Association (APA) guidelines for treatment of TD if, regardless of severity, it has an impact on the patient.
After Laura's TD diagnosis, the clinician educates Laura on TD and how it can be caused by exposure to APDs. He proposes treatment with a VMAT2 inhibitor. After learning that TD was caused by her APD, Laura wants to discontinue the atypical APD for both her and her daughter. She is also hesitant to start a new treatment, knowing that the previously prescribed medication caused her TD.
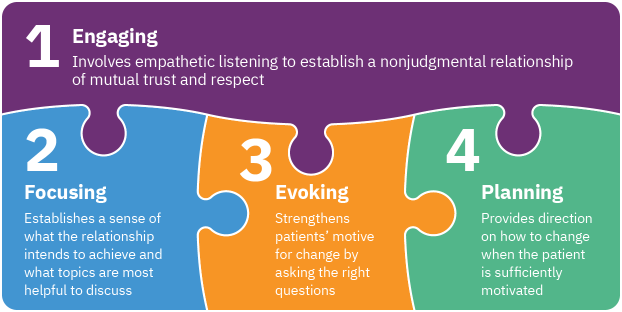
In the interest of supporting Laura's mental health needs and treating her TD, Laura's clinician addressed her hesitancy to start treatment by applying the principles of motivational interviewing. The key interactive elements of motivational interviewing are engaging, focusing, evoking, and planning (Figure 3).
Following 3 months of motivational interviewing focused on Laura's interest in achieving attainable goals, the clinician addressed her hesitancy to start treatment. Laura initiated a VMAT2 inhibitor for the treatment of her TD symptoms and continued treatment with the atypical APD.
After 3 months of treatment, Laura's symptoms have improved. Her AIMS score has decreased from 7 to 4. Laura is able to maintain her atypical APD and lithium. Her psychiatric symptoms are stable, she continues to work, and she once again feels comfortable meeting friends and family.
Laura was at greater risk for developing TD due to long-term exposure to atypical APDs and diagnosis of a mood disorder. After observing Laura's movements and listening to her concerns about the impact on her life, the clinician recognized her symptoms and performed an AIMS exam; based on visual assessment and the DSM-5-TR criteria for TD, Laura's clinician diagnosed her with TD.
The impact of TD can be substantial in patients with a mood disorder, even if their symptoms are subtle, and may not be perceived at the same level by HCPs. TD should be top of mind for all patients receiving APDs for treatment, especially those with a mood disorder. The APA recommends treatment with a VMAT2 inhibitor for TD that has an impact on the patient, as was the case with Laura.
In addition, TD can affect the management of the underlying mental health disorder not only for the patient but also for other individuals the patient knows who are receiving treatment for a mental health disorder. For example, Laura wanted both herself and her daughter to discontinue treatment with an APD because it caused her TD.
Laura's case highlights the importance of keeping TD top of mind when managing patients with mood disorders. It underscores the necessity of observing and asking about involuntary movements at every clinical encounter with patients taking APDs, as the impact of even subtle TD can be extensive. TD, regardless of severity, should be treated if it has an impact on the patient. In addition, this case illustrates the importance of motivational interviewing in addressing a patient's hesitancy to initiate treatment of TD with a VMAT2 inhibitor.
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision. Washington, DC: American Psychiatric Association; 2022.
American Psychiatric Association. The American Psychiatric Association Practice Guideline for the Treatment of Patients With Schizophrenia. 3rd ed. Washington, DC: American Psychiatric Association; 2021. Accessed April 19, 2024. https://psychiatryonline.org/doi/pdf/10.1176/appi.books.9780890424841
Caroff SN, Citrome L, Meyer J, et al. A modified Delphi consensus study of the screening, diagnosis, and treatment of tardive dyskinesia. J Clin Psychiatry. 2020;81(2):19cs12983.
Data on file. Teva Neuroscience, Inc. Parsippany, NJ.
Fahn S, Jankovic J, Hallett M. Principles and Practice of Movement Disorders. 2nd ed. Philadelphia: Elsevier Saunders, Inc; 2011.
Finkbeiner S, Leo S, Goldschmidt D, et al. Differences in patient and healthcare professional perspectives on the key impacts of tardive dyskinesia. Presented at: XXVIII World Congress on Parkinson's Disease and Related Disorders; May 13-16, 2023; Chicago, IL.
Guy W. ECDEU Assessment Manual for Psychopharmacology. Revised 1976. Rockville, MD: US Department of Health, Education, and Welfare; 1976:534-537. DHEW publication ADM 76-338.
Hauser RA, Meyer JM, Factor SA, et al. Differentiating tardive dyskinesia: a video-based review of antipsychotic-induced movement disorders in clinical practice. CNS Spectr. 2022;27(2):208-217.
Jackson R, Brams MN, Citrome L, et al. Assessment of the impact of tardive dyskinesia in clinical practice: consensus panel recommendations. Neuropsychiatr Dis Treat. 2021;17:1589-1597.
Jain R, Ayyagari R, Goldschmidt D, Zhou M, Finkbeiner S, Leo S. Impact of tardive dyskinesia on physical, psychological, social, and professional domains of patient lives: a survey of patients in the United States. J Clin Psychiatry. 2023;84(3):22m14694.
McCutcheon RA, Keefe RSE, McGuire PK. Cognitive impairment in schizophrenia: aetiology, pathophysiology, and treatment. Mol Psychiatry. 2023;28(5):1902-1918.
Miller WR, Rollnick S. Motivational Interviewing: Helping People Change and Grow. 4th ed. New York: The Guilford Press; 2023.
STABLE National Coordinating Council Resource Toolkit Workgroup. STABLE Resource Toolkit. Accessed May 23, 2024.
Zutshi D, Cloud LJ, Factor SA. Tardive syndromes are rarely reversible after discontinuing dopamine receptor blocking agents: experience from a university-based movement disorder clinic. Tremor Other Hyperkinet Mov (N Y). 2014;4:266.






