Patients treated with both first- and second-generation antipsychotic drugs (APDs) are at risk for developing TD,1,2 an often persistent and potentially debilitating disorder characterized by involuntary hyperkinetic movements of the face, trunk, and extremities.3 In a meta-analysis that examined the prevalence of TD in patients with APDs, approximately 1 in 3 patients treated with typical APDs and up to 1 in 5 patients treated with atypical APDs had developed TD.1 Besides exposure to APDs, other factors that increase the risk of TD include age (older than 55 years), female sex (especially postmenopausal women), substance use disorder, intellectual disabilities or central nervous system injury, clinically significant parkinsonism or akathisia, and mood disorder (Figure 1).4,5
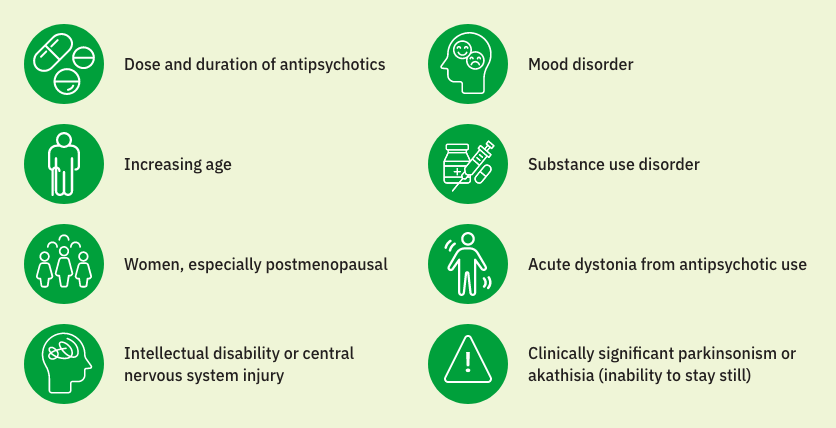
Mood disorders comprise a broad group of psychiatric conditions, including major depressive disorder and bipolar disorder, that affect the individual's emotional state and may include periods of excessive joy or sadness.6
In the United States, an estimated 43 million people suffer from schizophrenia and mood disorders, for which APDs are widely prescribed.7-13 From 2017 to 2022, the number of patients treated with atypical APDs increased by 22%, a rise primarily driven by its increasing use in patients with a mood disorder.2,14
Understanding the impact of TD is important for improving patient outcomes. Based on the underlying mental health disorder, patients may perceive the impact of TD differently. For example, patients with schizophrenia, who are more likely to have severe cognitive impairments, are often unaware of or unconcerned about abnormal movements of TD. Conversely, patients with a mood disorder, who otherwise may be highly functional and live active lives, can be bothered by even subtle TD symptoms and find them extremely disruptive.15,16
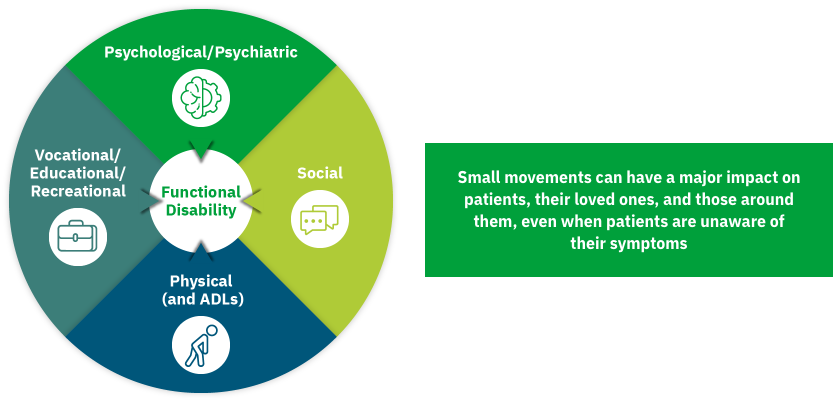
Irrespective of severity, TD can have a profound impact on many aspects of patients' lives.17 In a recent online survey of 269 patients with TD, 3 of 4 patients reported that the impact of TD was severe.18 Patients reported the impact of TD across 4 key domains (Figure 2)17:
Social
Physical
Psychological/psychiatric
Vocational/educational/recreational
No clinical studies have been conducted to evaluate the effects of treating TD on the outcomes listed.
The audio and video clips shown in Figure 3 are of a patient with depression and posttraumatic stress disorder who has been treated with an atypical antipsychotic for several years. They illustrate how subtle symptoms of TD can have a substantial impact on the patient. In Video 3a, when only hearing about the impact that TD symptoms are having on the patient, one would expect TD symptoms to be severe and obvious. However, when watching Video 3b, the symptoms are subtle and can be easily missed if the clinician is not observing the patient carefully. In Video 3c, the absence of sound makes TD movements more obvious, as the focus here is on seeing versus listening to the patient. This example underscores the importance of observation, even in the psychiatry setting, where patients and clinicians are largely focused on dialogue.
Video 3a
Video 3b
Video 3c
In 2020, an advisory panel of 7 experts assembled by Teva developed consensus recommendations on the need to assess the impact of TD on various domains in a patient’s life. A total of 6 recommendations were developed, of which 4 were related to assessing the impact of TD.19
Impact recommendation 1: importance of assessing19
Assess the impact of TD on the patient's life to guide TD treatment recommendations and aid TD treatment.
The impact of TD should not be based solely on the severity of abnormal movements
The degree of impact determines the level of treatment urgency
Information should be garnered from multiple sources, including staff and caregivers, all of whom may have valuable insights into how the patient is affected
Impact recommendation 2: key domains19
Assess the overall impact of TD on the individual's life and functioning in the social, physical, vocational, and psychological/psychiatric domains.
Impact recommendation 3: time points for assessing19
Assess the impact of TD at every patient visit because the impact varies over time and can affect treatment decisions.
Impact recommendation 4: approaches to assessing19
Utilize the key domains identified in recommendation 2 to assess the social, physical, vocational, and psychological/psychiatric impact of TD.
Consult with the patient directly and/or obtain input from caregivers/family/friends
Ask the patient questions related to disability; this can be especially helpful for understanding the impact of TD in patients with subtle symptoms, in whom abnormal movements may not be so obvious20
APA guidelines recommend that regardless of severity, TD symptoms that have an impact on the patient should be managed with a VMAT2 (vesicular monoamine transporter 2) inhibitor.4
Clinicians may, however, face several challenges in initiating treatment for TD and managing the underlying condition following a diagnosis of TD, especially in patients with a mood disorder who are highly functional. After learning that TD is an iatrogenic movement disorder (caused by their existing antipsychotic treatment), patients may make decisions that are counter to their well-being. These include becoming nonadherent or completely stopping their existing medication, discontinuing visits to their treating clinician, and advising others to not take their antipsychotic medication.18 In addition, these patients may be hesitant to consider taking a medication to treat TD, knowing that the condition was caused by their antipsychotic medication.
To address these issues, it is important that clinicians establish a dialogue with their patients at an appropriate time to educate on the need for, and safety and efficacy of, APDs in treating mood disorders or other underlying conditions. This also provides an opportunity to discuss the potential risks of TD as a side effect and the treatment options available to address the symptoms of TD.
Patients with a mood disorder may be more aware of their TD; therefore, it can have a significant impact, even when the movements are subtle. It is important to fully assess the impact of TD at every visit in patients with a mood disorder so that they can receive appropriate treatment.






