Tardive dyskinesia (TD) is one of several movement disorders caused by exposure to antipsychotics and other dopamine receptor blocking agents (DRBAs). It is critical to differentiate TD from other drug-induced movement disorders (DIMDs), particularly drug-induced parkinsonism (DIP), because anticholinergics which may be used to treat it can worsen TD. Through proper identification of TD, adequate and effective therapy can be provided to improve outcomes for patients.1
DRBAs, including both atypical and typical antipsychotics, are an important treatment option for potentially devastating psychiatric disorders like schizophrenia, bipolar disorder, and major depressive disorder.1 While these medications can be effective, they can also result in DIMDs.2
The term extrapyramidal symptoms (EPS) has been used broadly to describe all drug-induced abnormal movements and is still used by the US Food and Drug Administration (FDA) and among psychiatry providers. As our understanding of these conditions has evolved, the EPS term is now considered outdated as it fails to capture the distinct clinical presentations associated with individual DIMDs.1,3-5
Understanding the clinical presentation of common DIMDs can aid in the differential diagnosis (Figure 1).1
- TD is characterized by excessive and irregular movements, often affecting the face
- DIP is characterized by an overall paucity of movement but may also be accompanied by tremor
- Acute dystonia is characterized by pulling, twisting, sustained, and repetitive movements or postures
- Acute akathisia is characterized by a feeling of restlessness with an urge to move
ICD-10: G24.01*
ICD-10: G21.1
ICD-10: G24.02
ICD-10: G25.71
*The ICD-10 code G24.01 is for drug-induced subacute dyskinesia and is applicable to TD.
Because the EPS term is used broadly to describe motor symptoms linked with the use of DRBAs, anticholinergic medications, such as benztropine, were commonly prescribed to treat any abnormal movements regardless of the underlying DIMD.1,3,4 While benztropine is indicated to treat DIP, it is not recommended for patients with TD because it can worsen symptoms.5,10,11 Despite this warning, misuse of anticholinergics for treating TD persists. Approximately 40% of healthcare professionals (HCPs) in psychiatry report prescribing benztropine to treat or prevent TD.12
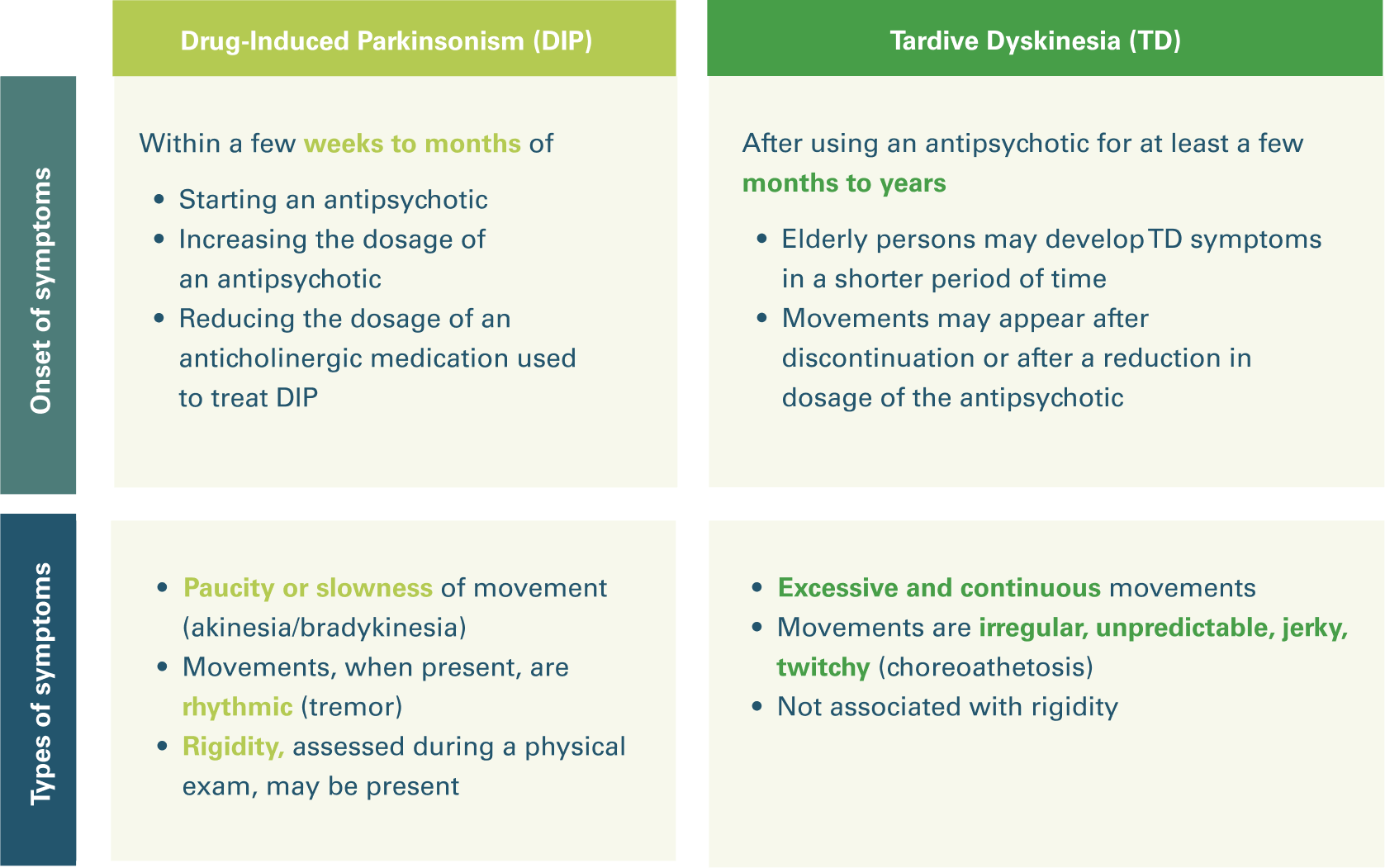
It is critical to differentiate between TD and DIP because the wrong treatment could lead to a worsening of symptoms.5,11 By understanding the key features that differ between TD and DIP, such as the timing of onset and the nature and frequency of movements, these disorders can be accurately identified (Figure 2).5,13 DIP typically develops within a few weeks to months of starting or after a dose increase of an antipsychotic and is characterized by a paucity or slowness of movements. When present, movements are rhythmic, and DIP may also be associated with rigidity.5,11,13,14 In contrast, TD typically develops after months to years of antipsychotic use. The minimum exposure history required for the diagnosis of TD is at least 3 months (or 1 month in patients aged ≥60 years). It is characterized by irregular movements that are jerky and unpredictable, without associated rigidity.5,11,13,15 Through careful assessment and differential diagnosis based on clinical presentation of the movements, HCPs can identify TD and ensure appropriate treatment is provided.1,16
TD is a chronic and irreversible condition.1 Although discontinuing the antipsychotic may improve or resolve the symptoms associated with DIP, antipsychotic reduction or complete withdrawal may fail to improve the symptoms of TD or might even induce withdrawal dyskinesia.5,11 Similarly, while anticholinergic medications, such as benztropine, are an appropriate treatment for DIP, they should not be used to treat or prevent TD because it may lead to worsening movements.5,11
The American Psychiatric Association (APA) recommends treatment with a VMAT2 inhibitor for TD that impacts patients' lives, but it should be noted that these agents can worsen parkinsonism.1,13 For patients with TD who are taking an anticholinergic, consider gradually reducing and discontinuing it and initiate treatment with a VMAT2 inhibitor when appropriate.5,17
- DIMDs have distinct clinical presentations and should have different approaches to treatment. This makes differentiating between movements essential for determining the appropriate treatment1
- Anticholinergics are not an appropriate treatment for TD and may exacerbate movements5,11
- TD and DIP differ in clinical presentation, timing of onset, and the nature and frequency of movements5,13
- DIP typically develops within a few weeks to months of starting or increasing the dose of an antipsychotic and is characterized by a paucity or slowness of movements. When present, movements are rhythmic, and DIP is often associated with rigidity5,11,13,14
- TD typically develops after at least a few months of antipsychotic use. It is characterized by irregular movements that are jerky and unpredictable5,11,13,15
- The APA recommends VMAT2 inhibitors for the treatment of TD that is impacting the patient17
1. Hauser RA, Meyer JM, Factor SA, et al. Differentiating tardive dyskinesia: a video-based review of antipsychotic-induced movement disorders in clinical practice. CNS Spectr. 2020;27(2):208-217. 2. Duma SR, Fung VS. Drug-induced movement disorders. Aust Prescr. 2019;42(2):56-61. 3. Miller JJ. Everyone please stop (EPS). Psychiatric Times. 2022;39(8). Accessed October 14, 2024. https://www.psychiatrictimes.com/view/everyone-please-stop-eps- 4. Ogino S, Miyamoto S, Miyake N, Yamaguchi N. Benefits and limits of anticholinergic use in schizophrenia: focusing on its effect on cognitive function. Psychiatry Clin Neurosci. 2014;68(1):37-49. 5. Ward KM, Citrome L. Antipsychotic-related movement disorders: drug-induced parkinsonism vs. tardive dyskinesia—key differences in pathophysiology and clinical management. Neurol Ther. 2018;7(2):233-248. 6. ICD-10 Data. 2025 ICD-10-CM Diagnosis Code G24.01. Accessed November 12, 2025. https://www.icd10data.com/ICD10CM/Codes/G00-G99/G20-G26/G24-/G24.01 7. ICD-10 Data. 2025 ICD-10-CM Diagnosis Code G21.1. Accessed November 12, 2025. https://www.icd10data.com/ICD10CM/Codes/G00-G99/G20-G26/G21-/G21.1 8. ICD-10 Data. 2025 ICD-10-CM Diagnosis Code G24.02. Accessed November 12, 2025. https://www.icd10data.com/ICD10CM/Codes/G00-G99/G20-G26/G24-/G24.02 9. ICD-10 Data. 2025 ICD-10-CM Diagnosis Code G25.71. Accessed November 12, 2025. https://www.icd10data.com/ICD10CM/Codes/G00-G99/G20-G26/G25-/G25.71 10. Benztropine mesylate tablet. Prescribing Information. Warren, NJ: Cipla USA, Inc. 11. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed, Text Revision. Washington, DC: American Psychiatric Association; 2022. 12. Chepke C, Benning B, Cicero S, et al. Investigating real-world benztropine usage patterns in movement disorders: claims analysis and health care provider survey results. Prim Care Companion CNS Disord. 2023;25(4):22m03472. 13. Psychiatry & Behavioral Health Learning Network. July 20, 2020. Q&A: updates from Dr Rakesh Jain on managing tardive dyskinesia. Accessed October 31, 2025. hmpgloballearningnetwork.com/site/pcn/article/qa-updates-dr-rakesh-jain-managing-tardive-dyskinesia 14. Patel T, Chang F. Practice recommendations for Parkinson's disease: assessment and management by community pharmacists. Can Pharm J (Ott). 2015;148(3):142-149. 15. Caroff SN. Overcoming barriers to effective management of tardive dyskinesia. Neuropsychiatr Dis Treat. 2019;15:785-794. 16. Guy W. ECDEU Assessment Manual for Psychopharmacology: Revised. Rockville, MD: US Department of Health, Education and Welfare, Public Health Service, Alcohol, Drug Abuse and Mental Health Administration, NIMH Psychopharmacology Research Branch, Division of Extramural Research Programs; 1976:534-537. DHEW publication number ADM 76-338. 17. American Psychiatric Association. The American Psychiatric Association Practice Guideline for the Treatment of Patients With Schizophrenia. 3rd ed. Washington, DC: American Psychiatric Association; 2021.